
Sinus Cancer LCR
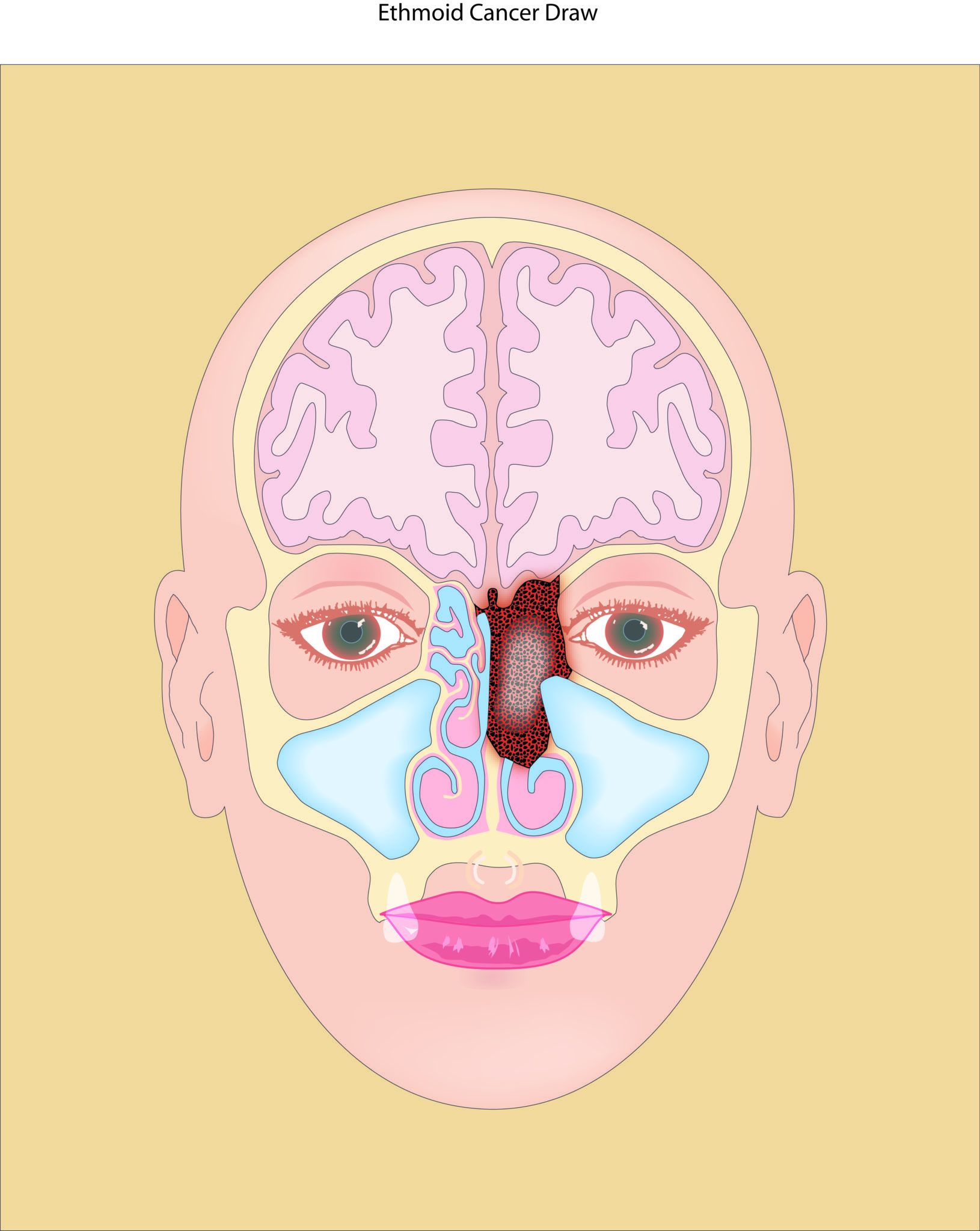
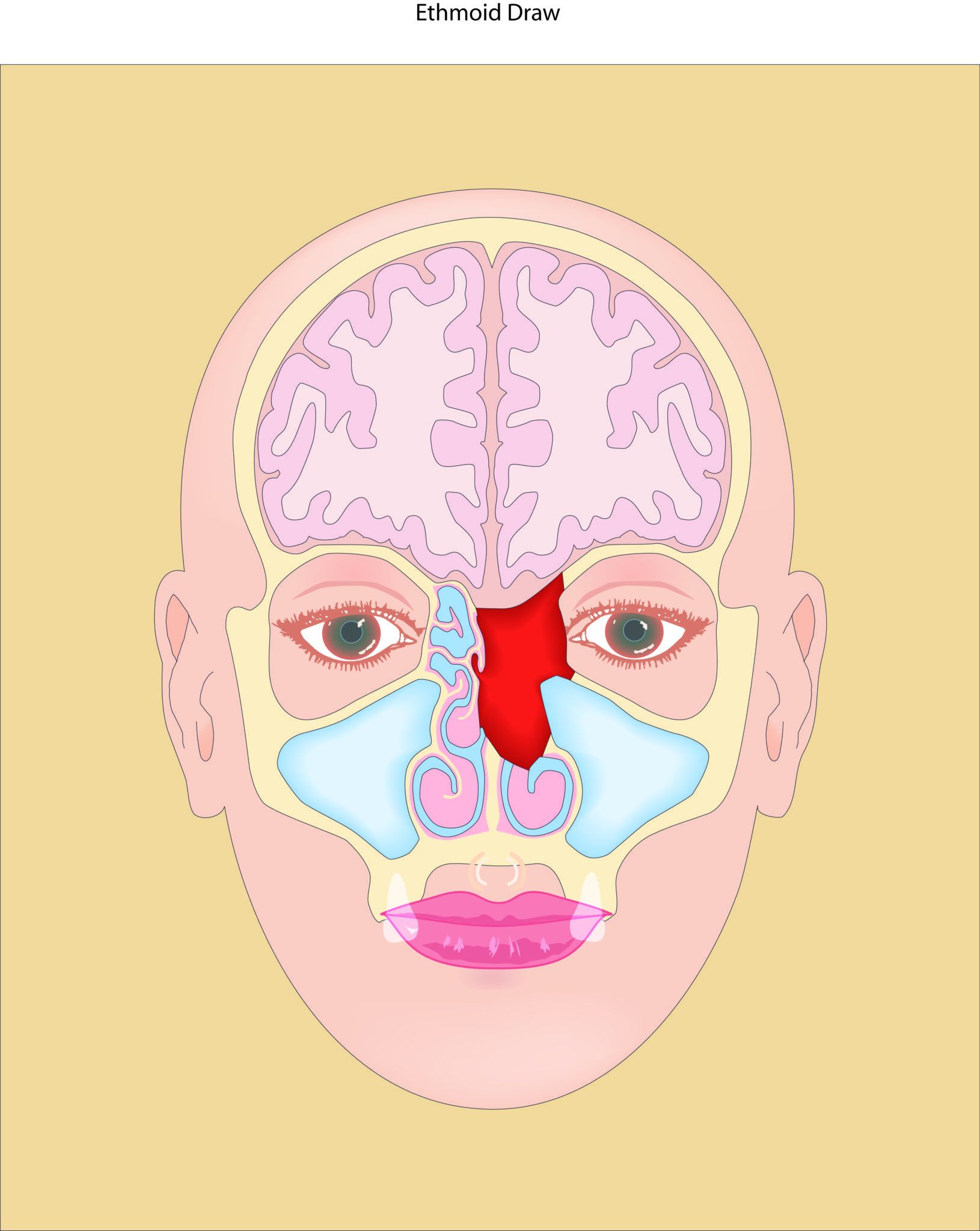
Cancers (malignancies) of the nasal cavity and sinuses represent less than 1% of all cancers. Their overall incidence is estimated to be 1 case / 200,000 people / year.1 In general, affects men more often than women (the ratio is 1.8:1). 2 The majority of sinus/nasal malignancies (80%) are diagnosed between the ages of 40-70 years but it can present in teenagers, children and even infants. The most common sites of involvement are the nasal cavity (43.9%) and maxillary sinus (35.9%) but they can also present primarily at the ethmoid, frontal or sphenoid sinuses. (See Figure 1)
The early diagnosis of sinus cancer is often delayed because symptoms can be dismissed as common everyday problems by patients and physicians. Some of the common early symptoms include unilateral nasal obstruction, nasal bleeding, headaches, loss of sense of smell or sinus infections. Advanced symptoms include severe pain, numbness or tingling of the face, abnormal tearing, double vision or visible asymmetry of the face or eyes. Diagnosis is made by a combination of physical examination with endoscope, radiological imaging and eventual pathological examination.
Treatment depends not only on the type of cancer but also the extension of the tumor and the status of metastatic lesions widespread. Three radiological imaging modalities are usually necessary. A CT scan provides information about the osseous components of the nose, orbit and skull base. It also provides the images for the stealth navigation system which is a Sinus GPS system use during endoscopic resection of these tumors. The MRI offers information about intracranial extension of the tumor to the dura or brain, perineurial invasion and orbital invasion. Finally, as many of these tumors are in an advance stage at the moment of diagnosis a PET CT contributes information about tumor metastasis.
Fortunately when aggressively treated, there are cancers cures. Treatment most often requires a multidisciplinary approach using the expertise of a Rhinologist Skull & Base Surgeon, a neurosurgeon, a microvascular/reconstructive surgeon, a radiation oncologist, and a medical oncologist. In general, the best treatment results are reported when patients are treated with surgery follow by radiation. However, induction chemoradiation may be advised before surgery.
About Sinus Cancer Surgery:
Surgery is recommended as part of a treatment plan that is intended to cure sinus cancer, to improve symptoms and to avoid disastrous complications. The primary goal is the removal of all visible cancer while maintaining quality of life. Surgery also has a palliative purpose by reducing pain, controlling nasal bleeding, and reestablishing nasal breathing. Nasal and sinus cancers can now be successfully removed by using a trans-nasal endoscopic approach, which means that the surgeon removes the tumor through the nose using special cameras and instruments and therefore avoids disfiguring face and head incisions.
1. Sinus Cancer Involving the Mouth: Maxillary sinus and nasal cavity cancers can erode downwards towards the roof of the mouth and involve the tooth roots or the palate. When this is a concern patients are advised to see a dentist or oral maxillofacial surgeon before proceeding with an intervention. Teeth that are in poor health need to be removed before beginning radiation therapy, otherwise they can be a source of serious jaw infections. If there is substantial involvement of the mouth by the cancer then the prosthodontist, can create a “dental impression” of mouth before surgery to build a denture device, called an obturator. The obturator is used to replace that part of the mouth that is at risk from cancer and to prevent food and liquids from passing from the mouth into the nasal airway when you eat.
2. Sinus Cancer Involving the Orbit (Eye Socket): Sinus cancers can erode into the eye causing pain, double vision, decreased vision or blindness. It can also block your tear duct and cause tearing from the eye and cheek numbness. Surgery for cancers involving the eye is tailored for each individual. The surgeon’s priorities are to preserve life first and vision as a second outcome. Dr. Tarrats offers advance orbital preservation techniques, however, sometimes cancer involving the eye is so extensive that surgery to remove the eye is advised as part of the treatment plan to cure it.
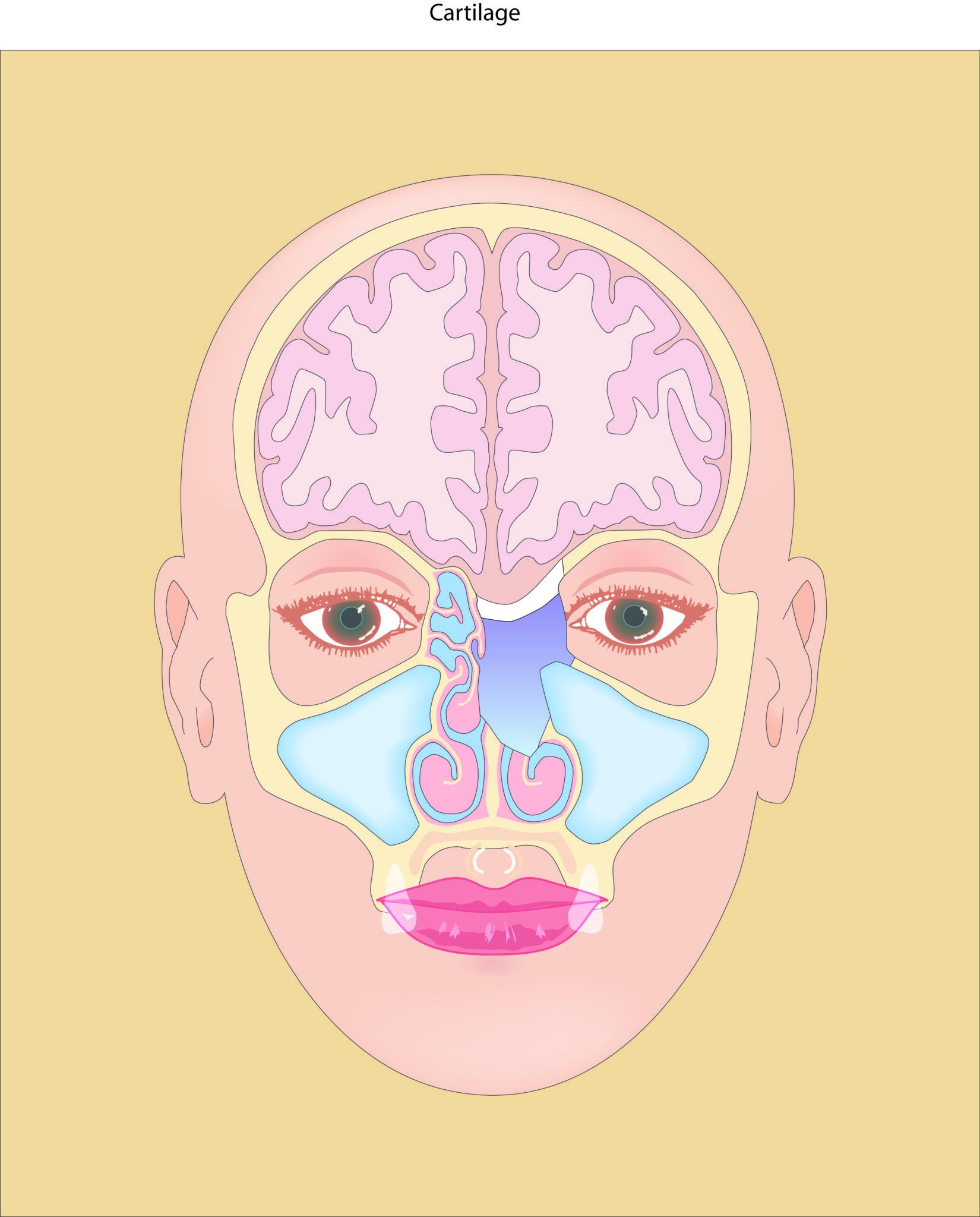
3. Sinus Cancer Involving the Skull Base/Brain: Sinus cancers can lie adjacent to the brain or even push up the brain from within the roof of the nasal cavity. With advent of endoscopic sinus surgery, we can approach many tumors through the nostrils using an endoscope (without the use of facial incisions). We do it in collaboration with a neurosurgeon who is the expert once we reach the intracranial compartment. After tumor resection to prevent brain herniation into the nasal cavity and to avoid intracranial infection, we reconstruct the skull base with tissues from other parts of the body like fascia latta, abdominal fat, ear cartilage or intranasal vascularized pedicle flaps.
The Five Most Common Sinus Cancers:
In the USA, the most common types are squamous cell carcinoma (51.6%) and adenocarcinoma (12.6%), followed by melanoma (6.6%) , esthesioneurobalstoma (olfactory neuroblastoma; 6.3%) and adenoid cystic carcinoma (6.2%). Cancers of non-sinus origins like lymphoma, breast cancer, and renal cell carcinoma can metastasized to the sinuses as well.
1. Squamous Cell Carcinoma is the most common cancer of the nasal cavity and sinuses. It is associated with tobacco exposure, nickel work, thorotrast, textiles (cotton, wool, and synthetic fibers), inverted papilloma and HPV infection in some people. Treatment may vary depending upon the extent of disease at initial presentation. Surgery is typically advised as an initial treatment followed by radiation with chemotherapy. Chemotherapy as a stand alone treatment for this type of cancer is seldom curative.
2. Adenocarcinoma Adenocarcinoma originates most often in the ethmoid sinuses near the area for sense of smell5 and has a strong association with wood dust exposure, chromium salt exposure and leather tanning materials and is considered an industrial disease. Hardwood types as ebony, oak and beech carry the greatest risk of developing sinonasal adenocarcinomas. Inhaling formaldehyde or substances normally used in this type of industry seems to further increase this risk. Treatment typically includes surgery as these are not highly “radiation sensitive” cancers. Postoperative radiotherapy is however considered part of appropriate treatment. There is also a positive effect of a chemotherapeutic agent called cisplatinum in some forms of adenocarcinoma.
3. Mucosal melanoma can present with dark, pigmented tissue which is a typical finding on endoscopy, although pigmentation is not always present. Sinonasal tract melanomas affect men and women equally. Mucosal melanoma is identified more frequently in black than white patients (10.4%).9 Melanosis (benign pigmentation in nasal lining) may be risk factors for the development of mucosal melanoma.10, 11, 12 Surgery and radiation are used as primary methods of treatment with chemotherapy reserved for cases of positive surgical margins, distant or disseminated disease and palliation. Radiotherapy may help local control but does not appear to affect overall cure.
4. Esthesioneuroblastoma (olfactory neuroblastoma) is believed to originate from neural tissue associated with sense of smell. Olfactory neuroblastoma equally affects men and women and can be found in all age groups. No known cause exists for this tumor. 15 Surgery and radiation are typically used with additional treatment to the lymph nodes in the neck. Up to 23.4% may develop cervical lymph node metastases.16 Thus, treatment of the clinically negative neck may be warranted. A combination of surgery and radiotherapy is the most frequently used approach, and the one that achieved the highest cure rates. Esthesioneuroblastoma is regarded in some cases to be sensitive to chemotherapy and is used as additional mode of therapy. Long term follow up for 10-20 years is advised.
5. Adenoid Cystic Carcinoma originates from minor salivary glands that are located throughout the nose and sinuses. Most patients are Caucasian (72.4%), non-smokers (48.4%), and non-drinkers (74.4%). The maxillary sinus (47%) and the nasal cavity (30%) were the most common primary tumor sites. This type of cancer typically involves perineural spread and bony invasion. Treatment consists of surgery followed by radiation, distant metastatic spread and late recurrence is more common than with other sinus malignancies. Radiotherapy is recommended to follow surgery since it seems to reduce local recurrence rates. In some individuals the progression of this type of cancer is very slow and recurrences can occur years to decades following initial treatment.
The Future
Unique technological advances, new surgical modalities, novel radiation therapies, recently developed chemotherapeutic agents and better diagnostic imaging are providing the necessary tools to triumph over sinonasal cancer. On March 4, 2017, at the North America Skull Base Society meeting in New Orleans Dr. Tarrats presented the sinus cancer experience of the Sinus & Nasal Institute of Florida where he did his fellowship. We proudly achieved a 90.3% local control on sinonasal malignancies treated with endoscopic surgery followed by proton beam radiotherapy. Those results represented the highest tumor local control ever achieved in the world. As we continue to improve we are hopeful that these outcomes will translate into better quality of life and longer survival for our patients.
